Fler deprimerade efter finanskrisen?

Q & A / Depression

1) Hejsan! Vilken bra sida:)..
Jag undrar vad det kan vara för fel om man är trött hela tiden. Jag är inte trött så jag somnar, men är trött generellt och har får pressa mig själv till att orka prata med folk ibland. Jag jobbar med människor och på grund av tröttheten blir jag väldigt disträ och klarar inte att konsentrera mig och det fungerar inte när man skall lyssna på någon annans problem. Jag vet att det inte beror på sömn för jag sover som regel 8-9 timmar varje natt. Någon annan sa också att det kan bero på att man har för lite B12 i kroppen. Vad kan det vara annars?? Tusen tack för svar:-)
/Pia
Answer:
Pia,
It is hard to tell why you are tired without a full evaluation, history and laboratory exams. The causes of tiredness or daytime fatigue are numerous. Some medical examples which I see frequently include anemia (low red blood cell count), hypothyroidism, sleep apnea, etc. The list of possible problems is very long. Vitamin deficiencies are on the list but are actually very rare in developed countries as long as someone has proper metabolism. For example, B12 deficiencies can be a result of decrease absorption in the gut.
I would not go spending my money on a bunch of vitamins now though. You should first see a general doctor for a medical work up. Following this, one could consider psychiatric causes of fatigue such as depression. There are also unknown or idiopathic causes such as chronic fatigue syndrome; these illnesses are thought to have a psychosomatic and medical component. There are many treatments out there for chronic fatigue but an accurate diagnosis of the problem should first be made. Go see your doctor and talk with him/her about your symptoms; blog back when you get some answers…..Dr. L
2)
Hej!Jag har en fåga till er Och jag vill gärna vara anonym.
Det enda jag vill här i livet är att vara lycklig. Och det går inte. Visst måste livet ha sina motgångar. Men mitt problem är att jag snöar in på vissa saker att oroa mig för. Och så kan jag inte sluta tänka på det.
Sen är jag lycklig ett tag tills jag hittar ett nytt problem att snö in på. Jag vill leva i nuet.....Läse i mia törnbloms bok och det är så klockrent - om du oroar dig för famtiden och har ångest för det som hänt så pissar du på nuet. Något i den stilen va det. Min man som är en väldigt förstående man brukar fråga mig om jag inte bara kan va lycklig???
Som i sommras gifte vi oss, då tror jag att något dålig måste hända för jag är typ glad.....Vaför kan jag inte bara ta dagen so den kommer oh vara lykligt. Det är ju supersvårt att vara lycklig.
Sen städar jag som en tog och jag vet att det är ångest dämpade.....
MVH miss C
Answer:
Hi miss C,
There are two forms of anxiety or stress. The first is what I call signal anxiety. It is there to warn us of appropriate danger, get us motivated to do the right thing, and keep us living and playing well with others. For example, if I am running late for work tomorrow morning, I should be worried---That way I will hurry and I will be apologetic to my boss in an appropriate manner---And, I will take future precautions that it not happen again.
The second kind of worry is pathologic worry or anxiety. This is what you are suffering from. Pathologic anxiety is worrying for the sake of worrying. Chronic anxiety results in very high rates of depression. There are medications to help with anxiety and they are pretty effective (60-70% response rate). These meds are called selective serotonin receptor inhibitors or SSRI’s. They are very safe in general and here in the U.S. it is given out like candy so many people are on them.
People with your form of anxiety were previously described as neurotic by Freud and others. This type of anxiety if very responsive to psychotherapy. And I would think that is the first best step; Access a good therapist that is not weird and that you feel comfortable with. Preferably one who specializes in Cognitive behavioral therapy (called KBT in Sweden), interpersonal therapy or psychodynamic psychotherapy. These are all good types of psychotherapy for the condition you describe. Freud said the goal of therapy is to learn to live and to love. A therapist could aid you in your quest….Dr. L
3)
Hej, först och främst. Vilken bra idé att skapa en blogg som verkligen kan hjälpa andra människor! Sen speciellt intressant då jag har en fråga som "plågat" mig sen sommaren 2006.
Jag har sedan jag var barn, runt sju år, haft återkommande depressioner och försökte när jag var tolv år ta mitt liv första gången. Periodvis mår jag skrämmande bra, utåt sett är jag lycklig. Men hösten 2005 då en vän till min bror tog livet av sig (17 år gammal) raserades mitt liv totalt. Jag mådde redan dåligt men blev efter begravningen helt "blockad", slutade äta och gick ner 13 kilo på lite mer än två månader. Ett par månader senare försökte jag ta mitt liv, överlevde som ni märker och sen gick det väl sådär. Jag började dricka mycket sprit, lekte med killars känslor bara för att själv må bättre. Sommaren 2006 träffade jag för första gången en psykolog via min kompis som ville ha in mig direkt.
Jag vägrade och flyttade hundra mil hemifrån. Jag träffade då min nv sambo och sedan dess har jag sällan varit ledsen, mått jättebra. Men är livrädd att det tar slut då han är min livlina. Psykologen menade på att jag kunde bli ännu sämre ifall jag drabbades av en ny depression då det bara blivit värre med åren. Men jag är livrädd att skaffa hjälp! jag tror stenhårt på självterapi.. Kan hon ha haft rätt? att om jag t ex blir ensam igen, kan det då leda till att min depression återkommer och att det kan bli värre än det varit? Jag är livrädd, jag har snart en universitetsutbildning och mängder av vänner.. men vet ju att en depression kan förstöra så mycket. Sen, funkar självterapi mot självmordstankar?
Långt, och kanske luddigt.. Ha det bra
Answer:
Your case is such that I do not wish to give advice. I do wish to give some background or psychoeducational stuff to help you. Suicidal thoughts occur in many people who suffer depression. A past history of depression during childhood and suicidal thinking with suicide attempt does make one high risk for relapse. While the past does not predict the future, it is the most predictive tool we in behavioral health have. Even though it sounds you are happy and doing well now, someone with your history should know all the developing signs of a reemerging depression. Read my earlier blog that way you have an idea of what depression looks like if it did ever start to come back.
Also, self therapy is a dangerous game because it has been shown that depression plays tricks on the brain’s ability to understand events in an appropriate context. Depression is like seeing the world through a kaleidoscope where only negative thoughts, images are allowed through. Better to build a relationship with someone who can be trusted and who has unconditional positive regard for you. Sometimes people can find this in their parents, less often friends. It is usually a mistake to depend on this in a partner.
One can always find positive regard in the right therapist. Unconditional positive regard is a basic service that we are paid to provide. If depression returns, it would be helpful to already have someone in place whom you can trust to help you see the world as it is, not the depressed version….Dr. L
Defining Clinical Depression / Betydelsen av klinisk depression.

There are many forms of depression and most have been defined clinically. It is important to understand the type of depression one suffers because this can greatly effect the determination of suitable treatment options and the progonosis of the depressive problem. For example, here are some clinical entities:
Adjustment disorder with depressed mood
Dysthymia
Substance induced mood disorder (alcohol and some other drugs can cause long term depression)
Bipolar depression
Major Depressive Disorder (MDD)
Major Depressive Disorder with psychotic features
Melancholic Depression
Atypical Depression
Depression not otherwise specified
As you can imagine it is not too helpful for someone with adjustment disorder (mild) try to compare or give advice on their feelings about depression to someone who suffers Melancholic Depression (a more severe form). It is similar to me having tension headaches and telling a friend with severe migraines that they just need to rinse their face with cold water and get a face massage.
Major depression generally evolves over weeks. With significantly depressed mood other biochemical changes may take place. Appetite, energy level, concentration, attention, sleep may all change as a result of depression. These types of changes is what we mean by "clinical depression" or Major Depressive Disorder (MDD).
Major Depressive Disorder is defined as a change of at least 5 out of 9 common symptoms lasting longer than 2 weeks with depressed or irritable mood. Symptoms include:
Mood (depressed or irritable)
Sleep (classically decreased with early morning wakening)
Appetite
Decrease interests
Guilty or feelings of worthlessness
Decreased energy
Decreased concentration
Psychomotor retardation or agitation
Suicidal thoughts or apathy.
*we have had many questions/comments on depression, I hope to respond to some of them tomorrow.
Godnatt for now .....Dr. Lacy
Veckans ämne: Depression

Att då och då känna sig ledsen, nedstämd, eller lite deppig är något som händer oss alla då tillvaron blir besvärlig, vilket är helt naturligt och har ingenting med sjukdom att göra. Våra känslor kommer oftast till ro efter en tid, kanske med hjälp och stöd av någon närstående klok person.
Ibland händer det emellertid att vi blir ledsna, deprimerade även när vi tycker att det inte finns någon tydlig orsak till detta. Vi har svårt att få saker och ting uträttade, ingenting är längre roligt, ingenting ger oss längre någon glädje, vi duger inte mycket till och framtiden ter sig mörk. Livsglädjen och vitaliteten försvinner. Nedstämdheten är både djupare och längre än vanlig vardagsdeppighet.

Depressioner medför ett stort lidande för den som drabbas. Utan behandling kan förloppet bli långvarigt. Trots att depressioner kan bli både djupa och långvariga, är behandlingsmöjligheterna goda. Det finns både psykoterapeutiska metoder (kognitiv terapi/KBT) och läkemedel som har bra effekt vid depressionstillstånd.
Vi hoppas på frågor och feedback från er. Om du har en ide till ett ämne, lämna gärna en kommentar och vi kommer göra vårt bästa för att informera om det som ni läsare tycker är intressant.
Parenting: The "Good-enough" Mother
Winnicott formulated and developed the idea of the good-enough mother. The good-enough mother is a mother whose conscious and unconscious physical and emotional attunement to her baby adapts to her baby appropriately at differing stages of infancy.
Three key aspects of the environment identified by Winnicott are holding, handling and object-presenting. The mother may thus hold the child, handle it and present objects to it, whether it is herself, her breast or a separate object. The good-enough mother will do this to the general satisfaction of the child. The good-enough mother tries to provide what the infant needs, but she instinctively leaves a time lag between the demands and their satisfaction and progressively increases it. As Winnicott states: "The good-enough mother...starts off with an almost complete adaptation to her infant's needs, and as time proceeds she adapts less and less completely, gradually, according to the infant's growing ability to deal with her failure" (Winnicott, 1953). The good enough mother stands in contrast with the "perfect" mother who satisfies all the needs of the infant on the spot, thus preventing him/her from developing.
The good-enough mother's behaviour can be described as the graduated failure of adaptation. Her failure to satisfy the infant needs immediately induces the latter to compensate for the temporary deprivation by mental activity and by understanding. Thus, the infant learns to tolerate for increasingly longer periods both his ego needs and instinctual tensions.
Winnicott sees the micro-interactions between the mother and child as central to the development of the internal world. After the early stage of connection with the mother and illusions of omnipotence comes the stage of relative dependence (objective reality) where children realize their dependence and learn about loss. The mother's failure to adapt to every need of the child helps them adapt to external realities. As the infant develops, the good-enough mother, unconsciously aware of her infant's increasing ego-integration and capacity to survive, will gradually fail to be so empathic. She will unconsciously "dose" her failures to those that can be tolerated, and the infant's developing ego is strengthened, the difference between "me" and "not-me" clarifies, omnipotence is relinquished, a sense of reality begins to emerge, mother can be increasingly seen as a separate person, and the capacity for concern can develop. This way the mother helps the child to develop a healthy sense of independence. Failure in this stage may result in the formation of a False self.
The trick of the good-enough mother is to give the child a sense of loosening rather than the shock of being 'dropped'. This teaches them to predict and hence allows them to retain a sense of control. Rather than sudden transition, this letting go comes in small and digestible steps, in which a transitional object may play a significant part.
The final phase of development, to independence, is never absolute as the child is never completely isolated. The mother's role is thus first to create illusion that allows early comfort and then to create disillusion that gradually introduces the child into the social world. Winnicott recognized that the child needs to realize that the mother is neither good nor bad nor the product of illusion, but is a separate and independent entity.
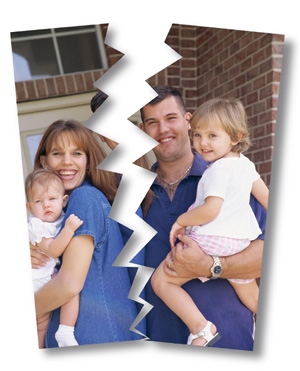
Studie säger splittrade familjer skadar barnen mer

Barn som växer upp i familjer med ensamstående föräldrar är dubbelt så vanligt som sina motsvarigheter för att utveckla allvarliga psykiska sjukdomar och missbruk senare i livet, enligt en viktig ny studie.
Forskare har i åratal diskuterat huruvida barn från splittrade familjer studsar tillbaka, eller om det är större risk att barn vars föräldrar vistelse tillsammans för att utveckla allvarliga känslomässiga problem.
Studien visar att ekonomiska svårigheter kan spela en roll, men andra experter säger att forskning stöder också uppfattningen att kvaliteten på föräldraskap kan vara en faktor.
I studien används det svenska nationella register, som täcker nästan hela befolkningen och innehåller omfattande socioekonomiska och hälsoinformation.
Forskarna fann att barn med ensamstående föräldrar var dubbelt så stor risk som andra att utveckla en psykisk sjukdom som depression eller schizofreni, att ta livet av sig eller försöker begå självmord, och att utveckla ett alkohol-relaterade sjukdomar.
Flickor var tre gånger större risk att bli missbrukare om de levt med en ensam förälder, och pojkar var fyra gånger högre risk.
Hela området är mycket omdebatterad och jag tycker det är mkt intressant att läsa om med tanke på att over 50 % av föräldrarna går separata vägar. Läs hela Artikeln här.
BTW, risken att ett skilsmässobarn skiljer sig som vuxen är dubbelt så hög jämfört med barn som inte upplevt en skilsmässa. Det visar två färska undersökningar. Läs mer.
Hur det står till med barnuppfostran i dagens Sverige?
Nannyboken innhåller också många konkreta tips som underlättar vardagen. Här finns checklistor och scheman, frågor och svar på mängder av vanliga frågor och inte minst Nannysarnas supertrick!
Q & A/ Barnuppfostran

Hur kan jag hjälpa mitt barn att utveckla en god självkänsla?
Min dotter fyller snart 8 år. Tack på förhand ;)
A:
Development (and maintenance ) of self esteem starts from a very young age and continues on into adulthood. By the time a child is latency age (5-9) much of the groundwork has already been laid down by parents and peers become increasingly more involved in one's self esteem.
Most adolescents have many struggles with self-esteem as they begin to obtain the cognitive ability to become more introspective and developmentally prepare for life on their own. It is very helpful for parents to understand child development in order to better assess their child's abilities and balance the parental need to be both supportive (nurturing) and demanding (increasing responsibility and accomplishments).
When discussing "self esteem" I think it helps to define two separate aspects. 1) self esteem 2) confidence. Many use these terms interchangeably but they are not one in the same.
1. Self-esteem = one's own inner feelings about themselves, their abilities, their attributes and their worth. The ability to feel good about one's self. LOVE
In general, when a person feels they are loved, liked, and cared for by those around them (friends, family, even acqaintances) they will develop growing self-esteem. "I am worthwhile". On the other hand, when a person feels unloved or rejected they will have diminishing self-esteem. "My boyfriend left me for another girl and I feel so ugly."
2. Confidence= the outward projection of behaviors, attitudes, appearances, and abilities. The ability to take on new challenges and appear capable to others. COMPETENCY
In general, when a person meets new challenges successfully they will develop growing confidence. "I always new that I could be famous". On the other hand, when a person is too anxious to bother taking new challenges or tries things too difficult resulting in failures they will have diminished confidence. "My mom never let me ride my bike outside the yard because she said it was too dangerous."
Parents should find ways to always remain fond of their children. Unconditional love (or the next best thing). Encourage relationships that enhance the love/adoration that is recieved. Discourage those that appear problematic or emotionally abusive.
Parents should struggle to find the right balance of pressing their child to "go for it" when there is a good chance for success and not be overly anxious about their child's ability/safety. At the same time, parents should avoid exaggerating pressure in areas the child is either unlikely to accomplish or has no desire or gain in accomplishing. With parental guidance and knowledge of a child's abilities, achievements and failures should appear more like a well balanced gungbräda. than an erratic one in which there is high risk of injury...Dr. Lacy
Charlotte:Jag tror barn behöver mycket stöd och kontakt med sina föräldrar för att utveckla en bra självkänsla. Detta genom att finnas dar med hjälp och stöd när det behövs, respektera barnets personliga integritet, erbjuda ditt barn tid tillsammans med dig varje dag, ( läsa en saga...) försök att förstå varför barnet känner olika känslor, och visa att du förstår, ge ditt barn friheten att utveckla en känsla av att han/hon kan klara av vad som helst bara viljan finns där, och uppskatta barnets uttryck för skapande tänkande och personlig problemlösning. Lycka till
Perfekta föräldrar finns inte

Att fa barn är en omvälvande process och man upptäcker tidigt att barnuppfostran är en svår men viktig del av vardagen. Jag tror att bli föräldrar är en av de största omvälvningarna som vuxna människor går igenom. Det tog mig några månader att komma in i mammarollen. Vår son ar idag 6 månader gammal och jag lär mig ngt nytt varje dag.
Barn kommer till världen fullständigt utlämnade och kräver av oss som föräldrar kärlek, uppmärksamhet och omtanke. Det låter självklart, men när man stupar av trötthet är det värt att påminna sig själv.
Barnuppfostran är ett omdiskuterat ämne och idag finns fler råd, uppfattningar och debatter om barnuppfostran än någonsin tidigare. Som forälder kan man lätt känna sig förvirrad om vad som ar "rätt"och "fel."
Alla barn har sina individuella behov och alla familjer har sin unika sammansättning. Men jag tror att en del saker är ändå av grundläggande betydelse för samspel och uppfostran:
• Den positiva inställningen till barnet.
• Förmågan och viljan att förmedla kärlek och glädje.
• Respekten för barnet och barnets känslor.
Uppfostran handlar om att stödja barnets utveckling. Även gränssättning, konsekvenser och rutiner måste ses i ljuset av detta.l
Visst låter det enkelt men vi vet alla att vi inte klarar att vara lika uppmärksamma hela tiden. Ibland saknas det energi, ibland räcker inte tiden till.
Det bästa ar nog att följa sin egen intuition och föregå med gott exempel. Jag tror även att det är väldigt viktigt som förälder att mitt i all barnuppfostran ta tid för dig själv och relationen. Hur ni som individer mår och er relation till varandra präglar barnet. Känner ni er tillfreds med er själva så har ni också mer att ge till ert barn.
Har du tips och idéer om barnuppfostran?
Lämna gärna en kommentar eller en fraga.
Har ny föräldrakultur gjort våra barn till mesar?
”Spring inte på trottoaren, hoppa inte två på studsmattan, gå inte så nära kanten.” Hör du dig själv? Den ständigt ängslige föräldern. Barnpsykologen Malin Bergström talar med aftonbladet om hur du kan släppa på kontrollen. Intressant artikel.
Barnuppfostran/The 5 F’s of good parenting
I decided to start off discussing the topic of good parenting with a conceptual framework my mentor taught me during Child and Adolescent Psychiatry fellowship training. I don’t know if he made it up or stole it from somewhere. And I can’t claim scientific validity. I can say it is an excellent framework that uncovers most problem of parenting.
Fond (kärleksfull): A good parent must like their child. Notice I chose the term “like” over “love”. A parent can love their child but never display that they like them. Children respond very well to the pattern of positive attention created by fondness. “You are so smart!” “Look how cute he is!” “Can you believe how strong our son is?!” Over time, all the doting (as long as it is genuine) builds a sense of well being, self esteem, and confidence in the child and his/her abilities. From an early age, children learn to strive for these moments of parental pleasure like a gambler at a slot machine. Unfortunately, fondness comes from within and it can’t be forced or pretended. My mentor used to say that fondness is the hardest tool to give a parent.

Firm (bestämd): A good parent must not allow their fondness, insecurity, anxiety, personal life, etc overcome their ability to be firm when necessary. This generally becomes important during the time of “the terrible two’s” (when kids first learn to act out aggression) and continues on into adulthood. Being firm requires being present, aware and consistent. It involves requiring and modeling good behavior during disagreements with the child. It does not include acting out one’s own parental aggression in order to subvert the child’s will.
Flexible(flexibel): A good parent must adjust with the times. Many parents confuse being “Firm” with being rigid. Parents must be ever mindful of the child’s need to explore and develop. Every parent should know basic child developmental stages. An 11 year old and a 16 year old are vastly different in their desires and abilities. The parent must have the flexibility to positively respond to the ever-changing child.
Fun(lekfull): Parents should spend time with their children that is enjoyed by both parent and child. This is true even through the teenage years. There is always some common ground to find in which both parent and child can do activities together. When problems develop, many times this is long lost or been ignored. I have parents who do 2 hours of homework with their 7 year old everyday but haven’t done something fun with them for weeks. Children are not little adults; they need to play.

Frank(uppriktig): Parents must whenever possible be open and honest with their children. It is generally a mistake to hide problems from kids. I have found that there is an appropriate way for a parent to discuss just about any problem with a child. If a parent can not figure out the appropriate way, then that is why there are therapists to help. A parent should always lean toward honesty whenever possible. It has been my experience that children (especially teenagers) are unbelievably good at sniffing out a lie or a family “secret”. When a parent is confronted with this, the parent should model frankness. It will be reciprocated... Dr.Lacy
Veckans ämne / Vad är rätt i barnuppfostran?
This week we will discuss some of the evidence and mental health findings concerning effective parenting. Most parents use their own childhood and anecdotal experiences gathered through early adulthood as a guide. Unfortunately, many parents did not grow up with a proper blue print for effective parenting and may get lost with reactive thinking. “I don’t want to do what my father/mother did to me.” Others may at times over-identify with their own childhood. “Honey, I am spanking our child because I was spanked and I turned out well.”
This week’s topic, like our last, is so broad we will not cover a large part of it. Readers of the blog will learn a bit about what researchers have shown concerning parenting and some of the ongoing controversies as well. Charlotte will add a few personal touches. Feel free to add comments, personal stories/views, or ask questions.
Q & A
Svar:
Den är mkt svår att besvara eftersom personer har olika stor känslighet och benägenhet att utveckla depression.
Depression är ju en sjukdom med många orsaker, både fysiska och psykiska. Men vi vet att det är vanligt att man blir deprimerad av långvarig alkoholförbrukning. Likaså av vissa mediciner. En del personer är känsliga för ljusbrist och kan bli deprimerade under höst och vinter. Långvarig stress kan också utlösa depression hos vissa personer.
Du kan minska risken att bli deprimerad om man har sådan benägenhet, genom bra kost, regelbunden motion, gärna promenader när det är som ljusast på dagen. Tank pa att vara måttlig med alkohol och ta reda på om den medicin man får har depression som biverkan.
Läs har om Ansvarsfriskrivning / Disclaimer
Psychiatry and Game Theory
Some theorists propose that the concept of “mental illness” as we know it is a false paradigm. One may view society as individuals playing within a collective game. Each of individual is trying to maximize their potential and gain with minimal effort or suffering. Some individuals understand and play the rules of the game better than others. Problems therefore arise.
"The struggle for definition is veritably the struggle for life itself. In the typical Western two men fight desperately for the possession of a gun that has been thrown to the ground: whoever reaches the weapon first shoots and lives; his adversary is shot and dies. In ordinary life, the struggle is not for guns but for words; whoever first defines the situation is the victor; his adversary, the victim. For example, in the family, husband and wife, mother and child do not get along; who defines whom as troublesome or mentally sick?...[the one] who first seizes the word imposes reality on the other; [the one] who defines thus dominates and lives; and [the one] who is defined is subjugated and may be killed."…Szasz
Mental health disorders are medical metaphors describing incidents when the individual’s desires or behaviors are in conflict with society or nature. Problems of living such as depression, anxiety, and even psychosis exist to be sure. However, it is false to liken them to traditional medical diseases that should be “treated” by a medical doctor. Psychiatrists are similar to “soul doctors”, the successors of priests or shamans, who deal with the spiritual “problems in living” that have troubled people forever.
While people behave and think in ways that are very disturbing, this does not mean they have a disease. Society’s definition of mental illness sometimes seems like a matter of semantics. Thomas Szasz, one of the leading psychiatrists of this view, wrote: "If you talk to God, you are praying; If God talks to you, you have schizophrenia. If the dead talk to you, you are a spiritualist; If you talk to the dead, you are a schizophrenic."

Through various Mental Health Acts or laws, psychiatry has slowly become a social control system, which disguises itself under the claims of scientificity.
It should be noted that Szasz’s views have been rejected by the American Psychiatric Association (APA) and the psychiatric establishment. His views are often inappropriately lumped in with less astute psychiatry deniers such as the Scientologists. While I disagree with much of his views, there is something compelling about them especially for any psychiatrist who has ever worked in military, forensic or disability evaluations. Dr. Lacy
Veckans Q & A
Har ni något råd till hur jag kan förklara bättre så han förstår.
A:
Manic depression, otherwise known as bipolar disorder, is a chronic life long condition marked by periods of euphoric highs and depressive lows. Roughly half of bipolar patients have lack of insight and do not realize they are ill. Poor compliance with treatment is common. Patients often feel a natural high during the manic phase and it is very difficult to convince them that they need a med to bring them down to reality. Generally, patients have better insight into the depressive phase of the illness and are willing to take meds to improve their depression.
I view the issue of compliance in bipolar much like that of drug or alcohol addiction. There is little that can be done until the bipolar patient proves to themselves that they have the disorder. This process can take years and usually occurs as a result of much personal damage. Like alcoholism, family members often learn to avoid the bipolar patient in order to escape the cycle of problems brought by untreated bipolar. As an example, over 90% of those married with bipolar undergo divorce. Sorry to be pessimistic but this is a very hard area for a family memer to improve. Here are some recommendations:
1. Try to be helpful and loving when your family member needs support but do not go way out of your way to help someone who must make a decision to help themselves.
2. Avoid offering finances to help. If helping this way pay for product directly.
3. Do not bother rationalizing with someone who is already manic; they must come down from mania before being rational.
4. Take advantage of the periods of normal mood (such as the period following mania) to help improve insight and maintain the relationship.
5. There is some data to suggest that the patient should build a long-term relationship with their psychiatrist and that family members should be invited into the treatment (if the bipolar patient is willing to let this happen). This way family members can report to the psychiatrist when the patient is beginning to cycle into depression or mania. Here is a link.
--Dr. Lacy

